- Welcome
- About
- Library
- Elections
- News
- Campaigns
- Standing Campaigns
- Governor-General Has Taken Sides
- Stop the Malik Report
- Don't Cancel Captain Cook
- Defend the Lord’s Prayer in the WA Parliament
- Labor Wants to Strip a Christian Church of Its Charity Status
- Thank the Coalition for Defending Christian Schools
- Tell MPs: Reform the Broken Sex Discrimination Act
- Tell Jim Chalmers: Stop the Reckless Spending
- Tell the Premier & Education Minister: No Teaching about Bestiality at School
- Thank Robbie Katter for Defending our Flag
- Your Home, Your Rights: Back Castle Law
- Thank Nigel Dalton for his vote to protect babies
- URGENT: Demand Justice for Baby Samuel!
- Reform Parliamentary Travel Entitlements
- Thank Tim Nicholls for Reinstating the Puberty Blocker Ban
- Stop Late-Term Abortion Bill: Protect Employers from Funding Abortions
- Thank NT Chief Minister Lia Finocchiaro for banning gender-confused men from women’s prisons
- Urgent — Help Stop the Surrogacy Bill 2025
- Tell Jacinta Allan: Stop Protecting Sex Offenders
- We stand with Jacinta Price
- Call on Lia Finocchiaro to Protect Christian Schools
- Thank Amanda Camm for Standing Up for Women
- Tony Burke’s Double Standard: Silencing Voices, Welcoming Extremists
- Thank Andrew Hastie for Defending Our Flag
- Tell the Albanese Govt: Stop Paying Women for Killing Their Babies
- Thank Senator Antic for Standing Up for Truth
- Tell the Melbourne Royal Show: Stop the Bible Ban
- Ask Health Minister Mark Butler: What are you doing to stop sex-selection abortion?
- Protect the Blood Supply – Keep the Ban on Gay Men Donating
- Tell the Liberals: Support Income Splitting for Families
- Tell The Nationals: Scrap Net Zero
- Tell Sussan Ley: Save Women’s Sport
- Thank Senator Henderson and the Coalition for Opposing University Indoctrination
- Tell Jim Chalmers: Drop the Woke $5 Note and Keep the Monarchy
- Thank Qantas Chairman John Mullen for Rejecting Corporate Wokeness
- Thank the NT Government for Protecting Free Speech and Religious Freedom
- Tell Chris Minns: Defund the Offensive Mardi Gras
- BREAKING NEWS! Midwives are being turned into abortionists
- Protect Our Schools from Political Activism
- Axe the Daniel Andrews Statue
- Thank the QLD Premier and QLD Health Minister
- Tell Premier David Crisafulli: Stand for Democracy in QLD – Restore the Right to Debate
- Emergency: Tell Key Senators to stop ‘Digital Prison’ Misinformation Bill
- Thank Peter Dutton for Commitment to Stand United Under One Flag
- Thank QLD Premier for Scrapping the “Truth-telling” Inquiry
- Where is the Honour and Respect for our King?
- Thank Toyota for Ditching Sponsorship of LGBT Parades and Events
- Protect Free Speech: Stop the Misinformation Bill
- Tell the AFL: Axe the ‘Welcome to Country’
- Tell Jim Chalmers: Don’t Ask Creepy Sex Questions on the Census
- Tell Jacinta Allan: Stop Radical Gender Indoctrination in Libraries
- Urgent Action On Babies Born Alive
- WA: Hit pause on dangerous gender self-ID bill
- A Fair Go for Families in Education
- Tell the Australian Olympic Committee: Ensure Respect for Christianity at the 2032 Brisbane Olympics
- Stop the Dangerous New “Human Rights Act”
- Stop Government-Mandated Radical Doctrines in Childcare
- Thank Bill Shorten for No More Prostitutes on the NDIS
- Repeal the Digital ID Bill to Protect Our Freedoms
- Tell the ADF: Stop the woke garbage and get serious about defending our nation
- Ask the Nationals to Support the Family with Income Splitting
- NSW: Stop the Inequity Bill
- Demand Answers from Labor MP Aaron Harper on the Babies Born Alive Bill Inquiry delay
- Defund the ABC over ‘racist country’ smear
- Tell the Premier and Opposition Leader: Keep Art Galleries Safe for Children
- Protect the rights of Biological Females
- Thank Cumberland City Council for Upholding Community Standards
- Tell Anthony Albanese the Bishop says Keep Free Speech
- Thank WA Liberals for ban on transgender drugs for kids
- Thank Anthony Albanese for his strong stand on Religious Freedom
- Thank Sarah Game for bill to prohibit gender ideology
- Thank the Opposition Leader and tell the Premier: Stop the Divisive Voice
- Tell the Premier & Education Minister: Kids should not be learning about bestiality at school
- Thank Archbishop Fisher for standing up for faith-based schools
- NSW: Tell NSW MPs: Oppose the flawed ‘Conversion Practices’ Bill
- Tell Peter Dutton: Protect Christian Schools
- Tell Mark Dreyfus To Keep Protections For Christian Schools
- Tell the PM & Opposition Leader: Protect Kids from Porn
- Tell Adelaide United: Free soccer star Musa Toure
- 27 WA Babies Cry Out From Their Graves
- Stop the Clandestine Censorship
- Keep the Monarchy on our $5 note
- Defund the ABC over Drag Queen activism
- VIC: Tell Victorian MPs: Keep the Lord’s Prayer!
- Hands Off Christian Schools
- Thank Peter Dutton for standing up for Australia Day
- Tell the PM: Stop the woke attack on Australia Day
- Thank the Coalition for their Policy to Keep Children Safe
- Tell the SA Premier: Hands off Anzac Day!
- Say No to Mutilating Healthy Body Parts
- Thank the ICC for banning gender confused men from women’s cricket
- Defend Religious Freedom In WA
- Thank Senator Antic for his bill to prohibit childhood gender transitions
- Federal babies bill must be voted on!
- Tell the Premier and Oppositiona Leader: Respect the Referendum - Repeal the SA Voice
- Thank Peter Dutton for calling for a proper Covid-19 inquiry
- Thank Peter Dutton for taking a stand against Hard Drugs
- Thank the AFL Commission for sticking to footy
- WA: Oppose the Deceiving WA Abortion Bill
- WA: Scrap The Shambolic Cultural Heritage Act
- Protect Children from Daycare Monsters
- Protect Unborn Children
- Tell MPs: Protect Freedom of Speech – Oppose the ACMA Disinformation Bill 2023
- Tell the PM: Protect Religious Freedom – Save Calvary Hospital
- Thank Monash council for cancelling drag queen story time
- Tell the Melbourne Comedy Festival: Reinstate Barry Humphries’ award
- Thank Dennis Hood, Sarah Game and Frank Pangillo for opposing woke language push
- Urge the PM to sack the Classification Board
- Support Henry Pike’s Bill to Save Australia Day
- Keep Moira Deeming MP in the Liberal Party
- Tell Adelaide City Council: Keep the Opening Prayer
- Thank the NRL for saying NO to gay ‘Pride Round’
- Tell Ch 10: Axe The Project over disgusting Jesus joke
- Tell the PM & AG: Protect the best interests of children
- Thank SA Libs for stand against the Voice to SA Parliament
- Thank Church Leaders for Protecting Christian School
- Protect Christian Schools
- Tell Albo: Keep your politics off the $5 note
- Thank Peter Dutton for No Blank Cheque on The Voice
- QLD: Do not attack parent rights and school choice
- Thank Senator Jacinta Price for opposing the divisive ‘Voice’
- Tell Mosman Council: Don't cancel Christmas!
- Thanks for Protecting Freedom of Speech
- Tell the SA Premier: Keep the Lord’s Prayer
- SA: Hands off the Lord’s Prayer
- NT: Stop attack on faith schools in the NT
- Keep using Mother and Father
- WA: Stop Zero Oversight To WA Emergency Powers
- Victoria – the Anti-Christian State
- WA: Defend Religious Freedom In WA
- Thank Anthony Albanese for keeping the Monarchy on our money
- Thank the Australian Catholic Bishops Conference for standing up to gender ideology
- QLD: Sophie's Law - Does the Queensland Government have a heart?
- Thank UAP Senator for standing up to radical identity ideology
- Stop abortion attack on religious hospitals
- Ask Albanese: When will you deliver $275 power bill cut?
- Stop the Killing in the Territories
- Keep opening the Senate with the Lord’s Prayer
- Coalition’s refreshing new voice of truth
- Tell the Manly Sea Eagles: Stick to footy - Ditch the LGBT propaganda
- Keep Christmas Day For Jesus
- Save Freo from “All Ages Drag Show”
- Tell MPs: We need a National Strategy to safeguard babies
- Say No to giving our Sovereignty away
- Say No to changing Birth Certificates in QLD
- Tell the woke NSW Premier: Keep the NSW flag – ditch the identity politics
- Introduce Miles Law to Protect Life in QLD
- QLD: Holding the QLD Premier to Account
- VIC: Andrews government divides children
- Adam Bandt disrespect for Australia, Australians and our Flag
- Keep Christian Chaplains in Schools
- Albanese to Ditch the Queen
- Keep Doors on School Toilets
- Tell the Breastfeeding Association: Do not cave to woke trans ideology
- Keep Blokes out of Women Sport
- Keep Australian Children Safe from Harms
- Mr Morrison - Can you help?
- Defund the UN over extreme abortion and gender ideology stance
- Tell Anthony Albanese: Protect Children from Trans Activists
- Protect Australians: Say no to hard drugs
- Stop Big Tech from Silencing Australians
- Tell MPs: Save Women’s Sport
- Time to Deliver on Religious Discrimination
- End Discrimination based on COVID19 Vaccination Status
- VIC: Act now to save Christian schools’ right to employ
- Tell MPs: Protect Free Speech
- Have your say in stopping kids’ access to online porn
- VIC: Act now to stop prostitution being decriminalised
- The ABC needs fixing
- WA: Free to Change: Stop McGowan’s therapy ban
- VIC: Act now to stop a second failed drug-injecting centre
- Act now to stop trans drugs for children
- Act now to stop Patten’s reckless changes to vilification laws
- Born Alive Bill
- Gambling Campaign
- Past Campaigns
- Events
- Contact
- 365Life
- Mother of the Year Awards
- Media Releases
- Little Music Church
![]()
YOUR GUIDE TO CURRENT ISSUES ON FAMILY, LIFE AND SOCIETY
 Donate
Donate Subscribe to our weekly newsletter to be kept up to date with the work FamilyVoice Australia is doing in our nation ![]()
-
Home

- News
News

FamilyVoice Australia will campaign nationally to ensure that the George Christensen private member's bill to require medical practitioners to provide, under law, a child born alive during a late term abortion with assured medical care.
The bill has been lodged by Federal Member for Dawson George Christensen, and seconded by the Member for New England Barnaby Joyce and is titled Human Rights (Children Born Alive Protection) Act 2021.
“The proposed bill will put in place a reporting requirement for medical practitioners to report children born alive as a result of abortion within seven days. It also underscores the false notion that the bill would require medical practitioners to provide life-saving treatments to non-viable babies” said Greg Bondar, spokesman for FamilyVoice Australia.
FamilyVoice is urging all members of parliament to ensure that a child born alive during a late term abortion remains alive. “The uncomfortable truth is that the child is left to die” added Greg Bondar.
The bill remedies the fact Australia is in breach of two international agreements to which it is a signatory: The Convention on the Rights of the Child, and the International Covenant on Civil and Political Rights, which recognise the right to life and the right of access to life-saving health care services.
FamilyVoice supports the bill’s offence provision when no life-saving treatment is provided with penalties of higher than $400,000 for health practitioners and higher for corporations. The bill, which could see health practitioners who breach the law deregistered in Australia, is a proper and appropriate sanction for doctors who fail to ‘save lives’.
FamilyVoice encourages and urges all Australians to lend their support for this bill via its website.

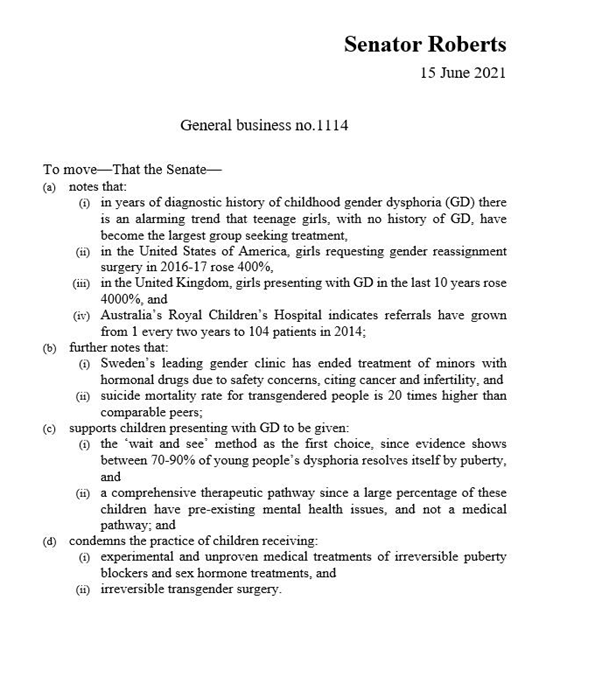
A motion by One Nation Senator Malcolm Roberts condemning transgender treatments on children has failed, with Coalition senators siding with Labor & the Greens to defeat it.
“The Liberals call themselves conservatives and today we have seen five liberal senators, including ministers, cross the floor to support Australian children accessing irreversible treatments and surgery,” said Senator Malcolm Roberts.
“My motion was about protecting children from these irreversible treatments at a time when a therapeutic pathway should take precedence over a medical pathway.
“It’s a travesty when we let children under 16 years have double mastectomies in Australia”, he said.
In Australia, children as young as 10 years of age have been prescribed puberty blockers.
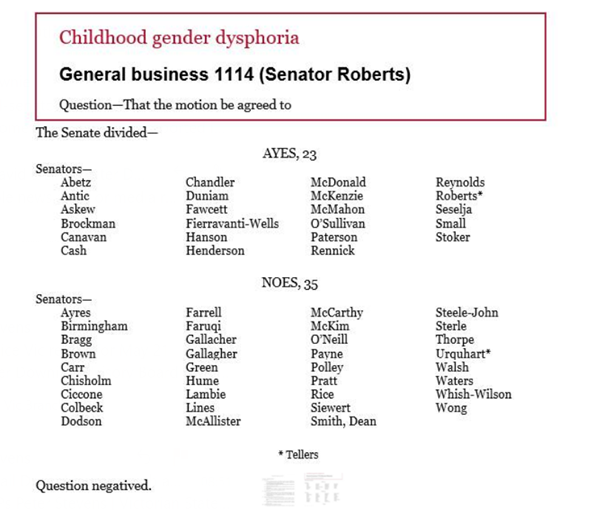
“It’s a sad day for all Liberal voters when their leader in the Senate, Simon Birmingham, crosses the floor and aligns himself with Labor and the Greens against the true conservatives in his party.
“The gang of five must be called to account for their sellout of conservative liberal values.
These are Senators Birmingham, Hume, Payne, Bragg and Colbeck.”
Speaking after the vote Senator Roberts said, “Adolescence is a confusing time and this is not the time for our children to make irreversible life changing decisions.
“It is no wonder that the Australian curriculum is loaded with anti-humanist, ideological rubbish when the former Minister for Education voted against my motion to protect children.
“Shame on him,” he said.
Liberal Senator Andrew Bragg was one of a number of Coalition senators who voted against the motion.
“We want to give people the maximum number of choices when they’re dealing with complicated issues as many trans people are. I think the idea that you would remove options like puberty blockers and other medical options from people is not appropriate,” Senator Bragg claimed.
“It’s not for politicians and the senate to be removing options from medical practitioners.
“I think it’s an inappropriate motion and I was pleased to see it defeated.”
Senator Bragg failed to mention that most children who suffer from gender dysphoria come to accept their real gender in time.
How Senators voted
A peaceful night vigil of hundreds of people at WA Parliament on June 16 will declare ‘No life is disposable at any time’ amid law changes that attack the safety of thousands of women and their children.
“Since we love all mothers and all their children, we reject the deceptive ‘Safe Access Zones’ Bill that threatens mandatory jail and huge fines for caring, silent offers of support to mothers,” said the rally organiser Darryl Budge, who is President of The Coalition for the Defence of Human Life.
“Mothers tell us that abortion leads to decades of pain and regret, and they wish they knew what damage it would do beforehand,” said the pro-life advocate who also represents FamilyVoice in WA.
“As a movement for life in WA, we mourn the deaths of 190,000 unborn children and the thousands of women who have been hurt since abortion was legalised in 1998.”
The WA government has a history of censoring offers of assistance to mothers in distress, according to Mr Budge.
“Amber-Jade Sanderson MLA has ordered the WA Health Department to delete pregnancy assistance groups like Abortion Grief Australia from the ‘Contacts’ section in three pregnancy-related Health Department brochures, even though the group employs qualified counsellors,” Mr Budge said.
“Ms Sanderson excused her discriminatory rejection of these three pregnancy assistance services in Parliament on November 10, by saying they were ‘religious’ and ‘outdated’.
“She did not explain why the government is already partnered with dozens of religious organisations to provide health, aged care, and welfare services.”
The WA government’s ‘Safe Access’ Bill will have a profoundly detrimental effect on the safety of distressed mothers, according to the Coalition for the Defence of Human Life, which is holding a large rally against abortion on June 16.
“The truth about abortion may be uncomfortable but the solution is not the criminalisation of communication about these matters,” said CDHL President Darryl Budge, who also represents FamilyVoice in WA.
“After helping a woman fleeing an abusive situation, a woman can be jailed and fined $12,000, due to this Bill, for having an abortion-related conversation in a 300-metre radius of an abortion facility,” said the father-of-two, who is co-chairing the annual Rally for Life at WA Parliament on June 16.
Mr Budge said that the bill dehumanises women’s independent capacity to protect themselves and their children from abuse at any point in their lives.
“It is distressing that a woman’s free choice to seek help during her pregnancy will be judged and barred by a court, not herself.
“In over 20 years, not a single vigil attendee has been arrested or moved on by police near an abortion clinic in WA.
“This unsafe bill is anti-woman and anti-child. It places women in harm’s way.”

FamilyVoice Australia upholds Christian values and the family: permanence of marriage, sanctity of human life, primacy of parenthood and limited government.
Subscribe to our award-winning publications!
Don't miss out on quality research and news that will equip you to face the culture wars.
Society is suffering from ‘progressive’ ideas.
Join the growing movement of young people daring to be counter-cultural.