- Welcome
- About
- Library
- Elections
- News
- Campaigns
- Standing Campaigns
- TAS: Let Tasmanians Speak
- Governor-General Has Taken Sides
- Stop the Malik Report
- Don't Cancel Captain Cook
- Defend the Lord’s Prayer in the WA Parliament
- Labor Wants to Strip a Christian Church of Its Charity Status
- Thank the Coalition for Defending Christian Schools
- Tell MPs: Reform the Broken Sex Discrimination Act
- Tell Jim Chalmers: Stop the Reckless Spending
- Tell the Premier & Education Minister: No Teaching about Bestiality at School
- Thank Robbie Katter for Defending our Flag
- Your Home, Your Rights: Back Castle Law
- Thank Nigel Dalton for his vote to protect babies
- URGENT: Demand Justice for Baby Samuel!
- Reform Parliamentary Travel Entitlements
- Thank Tim Nicholls for Reinstating the Puberty Blocker Ban
- Stop Late-Term Abortion Bill: Protect Employers from Funding Abortions
- Thank NT Chief Minister Lia Finocchiaro for banning gender-confused men from women’s prisons
- Urgent — Help Stop the Surrogacy Bill 2025
- Tell Jacinta Allan: Stop Protecting Sex Offenders
- We stand with Jacinta Price
- Call on Lia Finocchiaro to Protect Christian Schools
- Thank Amanda Camm for Standing Up for Women
- Tony Burke’s Double Standard: Silencing Voices, Welcoming Extremists
- Thank Andrew Hastie for Defending Our Flag
- Tell the Albanese Govt: Stop Paying Women for Killing Their Babies
- Thank Senator Antic for Standing Up for Truth
- Tell the Melbourne Royal Show: Stop the Bible Ban
- Ask Health Minister Mark Butler: What are you doing to stop sex-selection abortion?
- Protect the Blood Supply – Keep the Ban on Gay Men Donating
- Tell the Liberals: Support Income Splitting for Families
- Tell The Nationals: Scrap Net Zero
- Tell Sussan Ley: Save Women’s Sport
- Thank Senator Henderson and the Coalition for Opposing University Indoctrination
- Tell Jim Chalmers: Drop the Woke $5 Note and Keep the Monarchy
- Thank Qantas Chairman John Mullen for Rejecting Corporate Wokeness
- Thank the NT Government for Protecting Free Speech and Religious Freedom
- Tell Chris Minns: Defund the Offensive Mardi Gras
- BREAKING NEWS! Midwives are being turned into abortionists
- Protect Our Schools from Political Activism
- Axe the Daniel Andrews Statue
- Thank the QLD Premier and QLD Health Minister
- Tell Premier David Crisafulli: Stand for Democracy in QLD – Restore the Right to Debate
- Emergency: Tell Key Senators to stop ‘Digital Prison’ Misinformation Bill
- Thank Peter Dutton for Commitment to Stand United Under One Flag
- Thank QLD Premier for Scrapping the “Truth-telling” Inquiry
- Where is the Honour and Respect for our King?
- Thank Toyota for Ditching Sponsorship of LGBT Parades and Events
- Protect Free Speech: Stop the Misinformation Bill
- Tell the AFL: Axe the ‘Welcome to Country’
- Tell Jim Chalmers: Don’t Ask Creepy Sex Questions on the Census
- Tell Jacinta Allan: Stop Radical Gender Indoctrination in Libraries
- Urgent Action On Babies Born Alive
- WA: Hit pause on dangerous gender self-ID bill
- A Fair Go for Families in Education
- Tell the Australian Olympic Committee: Ensure Respect for Christianity at the 2032 Brisbane Olympics
- Stop the Dangerous New “Human Rights Act”
- Stop Government-Mandated Radical Doctrines in Childcare
- Thank Bill Shorten for No More Prostitutes on the NDIS
- Repeal the Digital ID Bill to Protect Our Freedoms
- Tell the ADF: Stop the woke garbage and get serious about defending our nation
- Ask the Nationals to Support the Family with Income Splitting
- NSW: Stop the Inequity Bill
- Demand Answers from Labor MP Aaron Harper on the Babies Born Alive Bill Inquiry delay
- Defund the ABC over ‘racist country’ smear
- Tell the Premier and Opposition Leader: Keep Art Galleries Safe for Children
- Protect the rights of Biological Females
- Thank Cumberland City Council for Upholding Community Standards
- Tell Anthony Albanese the Bishop says Keep Free Speech
- Thank WA Liberals for ban on transgender drugs for kids
- Thank Anthony Albanese for his strong stand on Religious Freedom
- Thank Sarah Game for bill to prohibit gender ideology
- Thank the Opposition Leader and tell the Premier: Stop the Divisive Voice
- Tell the Premier & Education Minister: Kids should not be learning about bestiality at school
- Thank Archbishop Fisher for standing up for faith-based schools
- NSW: Tell NSW MPs: Oppose the flawed ‘Conversion Practices’ Bill
- Tell Peter Dutton: Protect Christian Schools
- Tell Mark Dreyfus To Keep Protections For Christian Schools
- Tell the PM & Opposition Leader: Protect Kids from Porn
- Tell Adelaide United: Free soccer star Musa Toure
- 27 WA Babies Cry Out From Their Graves
- Stop the Clandestine Censorship
- Keep the Monarchy on our $5 note
- Defund the ABC over Drag Queen activism
- VIC: Tell Victorian MPs: Keep the Lord’s Prayer!
- Hands Off Christian Schools
- Thank Peter Dutton for standing up for Australia Day
- Tell the PM: Stop the woke attack on Australia Day
- Thank the Coalition for their Policy to Keep Children Safe
- Tell the SA Premier: Hands off Anzac Day!
- Say No to Mutilating Healthy Body Parts
- Thank the ICC for banning gender confused men from women’s cricket
- Defend Religious Freedom In WA
- Thank Senator Antic for his bill to prohibit childhood gender transitions
- Federal babies bill must be voted on!
- Tell the Premier and Oppositiona Leader: Respect the Referendum - Repeal the SA Voice
- Thank Peter Dutton for calling for a proper Covid-19 inquiry
- Thank Peter Dutton for taking a stand against Hard Drugs
- Thank the AFL Commission for sticking to footy
- WA: Oppose the Deceiving WA Abortion Bill
- WA: Scrap The Shambolic Cultural Heritage Act
- Protect Children from Daycare Monsters
- Protect Unborn Children
- Tell MPs: Protect Freedom of Speech – Oppose the ACMA Disinformation Bill 2023
- Tell the PM: Protect Religious Freedom – Save Calvary Hospital
- Thank Monash council for cancelling drag queen story time
- Tell the Melbourne Comedy Festival: Reinstate Barry Humphries’ award
- Thank Dennis Hood, Sarah Game and Frank Pangillo for opposing woke language push
- Urge the PM to sack the Classification Board
- Support Henry Pike’s Bill to Save Australia Day
- Keep Moira Deeming MP in the Liberal Party
- Tell Adelaide City Council: Keep the Opening Prayer
- Thank the NRL for saying NO to gay ‘Pride Round’
- Tell Ch 10: Axe The Project over disgusting Jesus joke
- Tell the PM & AG: Protect the best interests of children
- Thank SA Libs for stand against the Voice to SA Parliament
- Thank Church Leaders for Protecting Christian School
- Protect Christian Schools
- Tell Albo: Keep your politics off the $5 note
- Thank Peter Dutton for No Blank Cheque on The Voice
- QLD: Do not attack parent rights and school choice
- Thank Senator Jacinta Price for opposing the divisive ‘Voice’
- Tell Mosman Council: Don't cancel Christmas!
- Thanks for Protecting Freedom of Speech
- Tell the SA Premier: Keep the Lord’s Prayer
- SA: Hands off the Lord’s Prayer
- NT: Stop attack on faith schools in the NT
- Keep using Mother and Father
- WA: Stop Zero Oversight To WA Emergency Powers
- Victoria – the Anti-Christian State
- WA: Defend Religious Freedom In WA
- Thank Anthony Albanese for keeping the Monarchy on our money
- Thank the Australian Catholic Bishops Conference for standing up to gender ideology
- QLD: Sophie's Law - Does the Queensland Government have a heart?
- Thank UAP Senator for standing up to radical identity ideology
- Stop abortion attack on religious hospitals
- Ask Albanese: When will you deliver $275 power bill cut?
- Stop the Killing in the Territories
- Keep opening the Senate with the Lord’s Prayer
- Coalition’s refreshing new voice of truth
- Tell the Manly Sea Eagles: Stick to footy - Ditch the LGBT propaganda
- Keep Christmas Day For Jesus
- Save Freo from “All Ages Drag Show”
- Tell MPs: We need a National Strategy to safeguard babies
- Say No to giving our Sovereignty away
- Say No to changing Birth Certificates in QLD
- Tell the woke NSW Premier: Keep the NSW flag – ditch the identity politics
- Introduce Miles Law to Protect Life in QLD
- QLD: Holding the QLD Premier to Account
- VIC: Andrews government divides children
- Adam Bandt disrespect for Australia, Australians and our Flag
- Keep Christian Chaplains in Schools
- Albanese to Ditch the Queen
- Keep Doors on School Toilets
- Tell the Breastfeeding Association: Do not cave to woke trans ideology
- Keep Blokes out of Women Sport
- Keep Australian Children Safe from Harms
- Mr Morrison - Can you help?
- Defund the UN over extreme abortion and gender ideology stance
- Tell Anthony Albanese: Protect Children from Trans Activists
- Protect Australians: Say no to hard drugs
- Stop Big Tech from Silencing Australians
- Tell MPs: Save Women’s Sport
- Time to Deliver on Religious Discrimination
- End Discrimination based on COVID19 Vaccination Status
- VIC: Act now to save Christian schools’ right to employ
- Tell MPs: Protect Free Speech
- Have your say in stopping kids’ access to online porn
- VIC: Act now to stop prostitution being decriminalised
- The ABC needs fixing
- WA: Free to Change: Stop McGowan’s therapy ban
- VIC: Act now to stop a second failed drug-injecting centre
- Act now to stop trans drugs for children
- Act now to stop Patten’s reckless changes to vilification laws
- Born Alive Bill
- Gambling Campaign
- Past Campaigns
- Events
- Contact
- 365Life
- Mother of the Year Awards
- Media Releases
- Little Music Church
- Australian Christian Man of the Year Awards
![]()
YOUR GUIDE TO CURRENT ISSUES ON FAMILY, LIFE AND SOCIETY
 Donate
Donate Subscribe to our weekly newsletter to be kept up to date with the work FamilyVoice Australia is doing in our nation ![]()
-
Home

- News
News

Voted for the euthanasia bill (Bad vote):
David Basham, Finnis (Lib)
Frances Bedford, Florey (Ind)
Troy Bell, Mount Gambier (Ind)
Zoe Bettison, Ramsay (ALP)
Vickie Chapman, Bragg (Lib)
Matt Cowdrey, Colton (Lib)
Jon Gee, Taylor (ALP)
Eddie Hughes, Giles (ALP)
Steven Marshall, Dunstan (Lib)
Lee Odenwalder, Elizabeth (ALP)
David Pisoni, Unley (Lib)
Jayne Stinson, Badcoe (ALP)
Tim Whetstone, Chaffey (Lib)
Leon Bignell, Mawson (ALP)
Susan Close, Port Adelaide (ALP)
Fraser Ellis, Narungga (Ind)
Richard Harvey, Newland (Lib)
Paula Luethen, King (Lib)
Nick McBride, MacKillop (Lib)
Stephen Patterson, Morphett (Lib)
Carolyn Power, Elder (Lib)
Joe Szakacs, Cheltenham (ALP)
Corey Wingard, Gibson (Lib)
Blair Boyer, Wright (ALP)
Nat Cook, Hurtle Vale (ALP)
John Gardner Morialta (LIb)
Katrine Hildyard, Reynell (ALP)
Peter Malinauskas, Croydon (ALP)
Stephen Mullighan, Lee (ALP)
Chris Picton, Kaurna (ALP)
Rachel Sanderson, Adelaide (Lib)
Peter Treloar, Flinders (Lib)
Dana Wortley, Torrens (ALP)
*Geoff Brock, Frome (IND) - Did not vote but granted a pair in support of the bill.
Voted against the bill (Good vote):
Dan Cregan, Kavel (Lib)
Tom Koutsantonis, West Torrens (ALP)
Adrian Pederick, Hammond (Lib)
Vincent Tarzia, Hartley (Lib)
Sam Duluk, Waite (Ind)
Andrea Michaels, Enfield (ALP)
Tony Piccolo, Light (ALP)
Dan van Holst Pellekaan
Stephan Knoll, Schubert (Lib)
Steve Murray, Davenport (Lib)
David Speirs, Black (Lib)
*Michael Brown, Playford (ALP) - Did not vote but granted a pair against the bill.
Other
Note: Speaker Josh Teague (Heyson - Lib) did not vote.
Reconciliation with our Indigenous fellow citizens is incredibly important to most of us, as we recall the suffering of many Indigenous families over the past two centuries or more.
Here at FamilyVoice Australia we have a deep concern to reach out to the Indigenous community, and regularly give encouragement to Aboriginal children and adults.
But as Sydney Presbyterian pastor Mark Powell said in a recent Quadrant article, “Reconciliation starts with telling the truth.”
Mark has a degree in anthropology. He has studied several primary sources detailing Indigenous culture from the late 18th century, such as those summarised by noted anthropologist A.P. Elkin.
Mark says it’s difficult to see how true reconciliation can occur when falsehoods – such as claims that Aboriginal people lived in peace and harmony until the Europeans came – continue to be perpetrated.
So what were the actual beliefs and practices of Indigenous peoples living in Australia, especially since Europeans arrived?
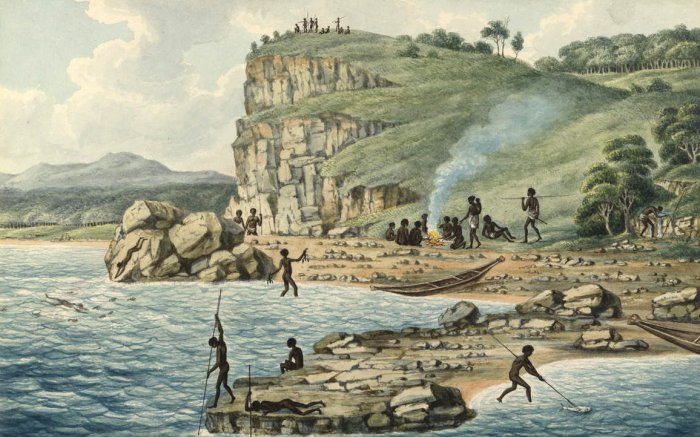
In his classic account published in 1964, The Australian Aborigines: How To Understand Them, Elkin describes how Indigenous communities treated their women. They were considered chattels, or worse. Some examples:
- Before a revenge expedition sets out on its dangerous enterprise, its members temporarily exchange wives, thus expressing their unity and friendship to one another.
- The final making of peace between two groups may always include the temporary exchange of wives, and on such occasions, all the usual tribal marriage laws (except those concerned with incest within the family) may be and are usually broken.
- Very often at times of great excitement during ceremonies, the men go aside to prearranged places and there have sexual intercourse with the women, and once again, the usual rules governing the intercourse of the sexes are ignored.
- These occasions are communal in nature, but there is another – the lending of a wife to a visitor.
Robert Hughes AO wrote the early history of British penal settlement in Australia, The Fatal Shore. He sought to provide an unvarnished snapshot of the cultural standards of that time, such as:
…the unalterable fact of [Indigenous] tribal life was that women had no rights at all and could choose nothing. A girl was usually given away as soon as she was born. She was the absolute property of her kin until marriage, whereupon she became the equally helpless possession of her husband. Before and after [marriage], she was merely a root-grubbing, shell-gathering chattel, whose social assets were wiry arms, prehensile toes and a vagina…
As a mark of hospitality, wives were lent to visitors whom the Iora tribesmen wanted to honour…. If a woman showed the least reluctance to be used for any of these purposes, if she seemed lazy or gave her lord and master any other cause for dissatisfaction, she would be furiously beaten or even speared.
There are many other accounts, such as one by escaped convict William Buckley. He lived for over 30 years among different Aboriginal groups, mostly in Victoria. In his story published in 1852, he reported that “violence, treachery, and killings” were common, almost everyday occurrences.
In many cases the conflicts began over sexual jealousy and abduction of women who, according to Buckley, were the “source of almost all the mischief in which the men engaged”.
Female Aboriginal skulls and bone fragments, uncovered and recorded by archaeologists and dated thousands of years old, had many more massive bone lacerations and scars compared with those in male skulls in the same burial site.
None of this evidence justifies the appalling treatment of Indigenous people by some white settlers.
But Australia’s Indigenous culture was far from idyllic before 1788. As Mark Powell says, true reconciliation cannot be achieved while historical falsehoods continue.
Peter Downie - National Director
FamilyVoice Australia


MPs across Australia must “get their act together” to protect more young people from the harms of gender intervention, argues FamilyVoice Australia.
“In response to a growing number of confused children and teenagers receiving puberty suppression or cross sex hormone intervention in various States, we respectfully urge MPs to get their act together and protect young people at risk from the harmful consequences of so-called gender identity treatment,” said FamilyVoice Australia spokesman David d’Lima.
Answers to questions recently raised in the West Australian Parliament by Hon Nick Goiran show a rapid increase in the number of confused young people receiving hormonal intervention in response to gender confusion.
“We commend Nick Goiran, but we need many more MPs to speak up and protect young people from life-long damage in the West and beyond,” David d’Lima said.
FamilyVoice also has applauded recent concerns raised in the New South Wales Parliament by Hon Fred Nile on the issue of gender intervention.
“Questions raised by Rev Nile have confirmed that the NSW Coalition Government supports experimental gender intervention on children that may produce life-long infertility and other irreversible consequences,” David d’Lima said.
“MPs who would not want such radical responses to harm their own young kids or grandchildren cannot sit back and allow confusion to somehow justify high risk prescriptions for young people in the mainstream community.
“The way forward is clarity about biology, and the sensitive encouragement of young people who are struggling with gender identity - but not to prescribe dangerous chemical intervention,” he said.
“MPs must also put a stop to the propaganda and misinformation about gender that is driving the confusion in the first place.”
These days, men and boys are in trouble.
Baptist pastor Murray Campbell recently wrote about one example close to his home. As he explained in the Eternity online newspaper, students at the co-ed Parkdale Secondary College were shocked by what happened a few weeks ago.
A female youth worker from the local city council had been invited to give a presentation as part of a “diversity and inclusion” program. According to eyewitness accounts, year 11 boys were “ordered to stand up in class”. What followed was anything but diverse and inclusive.
The Herald Sun reported that the boys were then “slammed by a council youth worker for being white, male and Christian ‘oppressors’”.
If the students were “white”, “male” and “Christian”, they were made to stand and face public humiliation as the youth worker “told them they were responsible for being ‘privileged’ and ‘oppressors’”.
A 16-year-old student said: “It was so messed up, we thought for a moment it was a joke, but then we realised it wasn’t and we were so upset and angry by it all.
“The youth worker basically said straight, white, Christian males were oppressors and they held all the power and privilege in society. The male students felt shamed and targeted.
“It was quite difficult to say anything because she was also talking about LGBTQI+. If you spoke out against that you feared you’d be called homophobic,” the student said.
Murray Campbell said such attitudes and ideas, deriding boys, heterosexuality and Christianity, are not new. “’Safe Schools and Healthy Relationships’ are now part of the curriculum in every Victorian government school and many private schools,” he said.
He could have added that parts of the Safe Schools program are still being taught in other states, including NSW and SA where it is officially banned.
Parkdale Secondary College is only the tip of the iceberg. There is a war against men being waged across the Western world, including Australia and the US, where the photo below was taken.
Feminist message above a mirror in a male bathroom
But social commentator Bettina Arndt has cited extensive research showing that in violent homes it’s not just the dad who is aggressive. Mothers are just as likely to be violent.
“Look at this important study from the Australian Institute of Criminology, which asked young people whether they’d ever witnessed their dads bashing their mums, or the other way around,” Bettina says.
“While the author, David Indermauer, trumpets the finding that almost a quarter of the kids had witnessed their fathers attack their mothers, he totally buries the most important result: almost the same percentage had seen their mothers attacking fathers.”
We are grateful to NSW Upper House MP Mark Latham, who has introduced a Parents’ Rights Bill to give parents a greater say in the moral values taught to their children. We believe all states should pass similar legislation.
And we also believe that Australian students deserve to know the truth – that neither women nor men are naturally peaceful and non-violent. Both sexes need self-control and respect for others.
As the Apostle Paul put it: “All have sinned.”
Peter Downie - National Director
FamilyVoice Australia
FamilyVoice Australia upholds Christian values and the family: permanence of marriage, sanctity of human life, primacy of parenthood and limited government.
Subscribe to our award-winning publications!
Don't miss out on quality research and news that will equip you to face the culture wars.
Society is suffering from ‘progressive’ ideas.
Join the growing movement of young people daring to be counter-cultural.