- Welcome
- About
- Library
- Elections
- News
- Campaigns
- Standing Campaigns
- TAS: Let Tasmanians Speak
- Governor-General Has Taken Sides
- Stop the Malik Report
- Don't Cancel Captain Cook
- Defend the Lord’s Prayer in the WA Parliament
- Labor Wants to Strip a Christian Church of Its Charity Status
- Thank the Coalition for Defending Christian Schools
- Tell MPs: Reform the Broken Sex Discrimination Act
- Tell Jim Chalmers: Stop the Reckless Spending
- Tell the Premier & Education Minister: No Teaching about Bestiality at School
- Thank Robbie Katter for Defending our Flag
- Your Home, Your Rights: Back Castle Law
- Thank Nigel Dalton for his vote to protect babies
- URGENT: Demand Justice for Baby Samuel!
- Reform Parliamentary Travel Entitlements
- Thank Tim Nicholls for Reinstating the Puberty Blocker Ban
- Stop Late-Term Abortion Bill: Protect Employers from Funding Abortions
- Thank NT Chief Minister Lia Finocchiaro for banning gender-confused men from women’s prisons
- Urgent — Help Stop the Surrogacy Bill 2025
- Tell Jacinta Allan: Stop Protecting Sex Offenders
- We stand with Jacinta Price
- Call on Lia Finocchiaro to Protect Christian Schools
- Thank Amanda Camm for Standing Up for Women
- Tony Burke’s Double Standard: Silencing Voices, Welcoming Extremists
- Thank Andrew Hastie for Defending Our Flag
- Tell the Albanese Govt: Stop Paying Women for Killing Their Babies
- Thank Senator Antic for Standing Up for Truth
- Tell the Melbourne Royal Show: Stop the Bible Ban
- Ask Health Minister Mark Butler: What are you doing to stop sex-selection abortion?
- Protect the Blood Supply – Keep the Ban on Gay Men Donating
- Tell the Liberals: Support Income Splitting for Families
- Tell The Nationals: Scrap Net Zero
- Tell Sussan Ley: Save Women’s Sport
- Thank Senator Henderson and the Coalition for Opposing University Indoctrination
- Tell Jim Chalmers: Drop the Woke $5 Note and Keep the Monarchy
- Thank Qantas Chairman John Mullen for Rejecting Corporate Wokeness
- Thank the NT Government for Protecting Free Speech and Religious Freedom
- Tell Chris Minns: Defund the Offensive Mardi Gras
- BREAKING NEWS! Midwives are being turned into abortionists
- Protect Our Schools from Political Activism
- Axe the Daniel Andrews Statue
- Thank the QLD Premier and QLD Health Minister
- Tell Premier David Crisafulli: Stand for Democracy in QLD – Restore the Right to Debate
- Emergency: Tell Key Senators to stop ‘Digital Prison’ Misinformation Bill
- Thank Peter Dutton for Commitment to Stand United Under One Flag
- Thank QLD Premier for Scrapping the “Truth-telling” Inquiry
- Where is the Honour and Respect for our King?
- Thank Toyota for Ditching Sponsorship of LGBT Parades and Events
- Protect Free Speech: Stop the Misinformation Bill
- Tell the AFL: Axe the ‘Welcome to Country’
- Tell Jim Chalmers: Don’t Ask Creepy Sex Questions on the Census
- Tell Jacinta Allan: Stop Radical Gender Indoctrination in Libraries
- Urgent Action On Babies Born Alive
- WA: Hit pause on dangerous gender self-ID bill
- A Fair Go for Families in Education
- Tell the Australian Olympic Committee: Ensure Respect for Christianity at the 2032 Brisbane Olympics
- Stop the Dangerous New “Human Rights Act”
- Stop Government-Mandated Radical Doctrines in Childcare
- Thank Bill Shorten for No More Prostitutes on the NDIS
- Repeal the Digital ID Bill to Protect Our Freedoms
- Tell the ADF: Stop the woke garbage and get serious about defending our nation
- Ask the Nationals to Support the Family with Income Splitting
- NSW: Stop the Inequity Bill
- Demand Answers from Labor MP Aaron Harper on the Babies Born Alive Bill Inquiry delay
- Defund the ABC over ‘racist country’ smear
- Tell the Premier and Opposition Leader: Keep Art Galleries Safe for Children
- Protect the rights of Biological Females
- Thank Cumberland City Council for Upholding Community Standards
- Tell Anthony Albanese the Bishop says Keep Free Speech
- Thank WA Liberals for ban on transgender drugs for kids
- Thank Anthony Albanese for his strong stand on Religious Freedom
- Thank Sarah Game for bill to prohibit gender ideology
- Thank the Opposition Leader and tell the Premier: Stop the Divisive Voice
- Tell the Premier & Education Minister: Kids should not be learning about bestiality at school
- Thank Archbishop Fisher for standing up for faith-based schools
- NSW: Tell NSW MPs: Oppose the flawed ‘Conversion Practices’ Bill
- Tell Peter Dutton: Protect Christian Schools
- Tell Mark Dreyfus To Keep Protections For Christian Schools
- Tell the PM & Opposition Leader: Protect Kids from Porn
- Tell Adelaide United: Free soccer star Musa Toure
- 27 WA Babies Cry Out From Their Graves
- Stop the Clandestine Censorship
- Keep the Monarchy on our $5 note
- Defund the ABC over Drag Queen activism
- VIC: Tell Victorian MPs: Keep the Lord’s Prayer!
- Hands Off Christian Schools
- Thank Peter Dutton for standing up for Australia Day
- Tell the PM: Stop the woke attack on Australia Day
- Thank the Coalition for their Policy to Keep Children Safe
- Tell the SA Premier: Hands off Anzac Day!
- Say No to Mutilating Healthy Body Parts
- Thank the ICC for banning gender confused men from women’s cricket
- Defend Religious Freedom In WA
- Thank Senator Antic for his bill to prohibit childhood gender transitions
- Federal babies bill must be voted on!
- Tell the Premier and Oppositiona Leader: Respect the Referendum - Repeal the SA Voice
- Thank Peter Dutton for calling for a proper Covid-19 inquiry
- Thank Peter Dutton for taking a stand against Hard Drugs
- Thank the AFL Commission for sticking to footy
- WA: Oppose the Deceiving WA Abortion Bill
- WA: Scrap The Shambolic Cultural Heritage Act
- Protect Children from Daycare Monsters
- Protect Unborn Children
- Tell MPs: Protect Freedom of Speech – Oppose the ACMA Disinformation Bill 2023
- Tell the PM: Protect Religious Freedom – Save Calvary Hospital
- Thank Monash council for cancelling drag queen story time
- Tell the Melbourne Comedy Festival: Reinstate Barry Humphries’ award
- Thank Dennis Hood, Sarah Game and Frank Pangillo for opposing woke language push
- Urge the PM to sack the Classification Board
- Support Henry Pike’s Bill to Save Australia Day
- Keep Moira Deeming MP in the Liberal Party
- Tell Adelaide City Council: Keep the Opening Prayer
- Thank the NRL for saying NO to gay ‘Pride Round’
- Tell Ch 10: Axe The Project over disgusting Jesus joke
- Tell the PM & AG: Protect the best interests of children
- Thank SA Libs for stand against the Voice to SA Parliament
- Thank Church Leaders for Protecting Christian School
- Protect Christian Schools
- Tell Albo: Keep your politics off the $5 note
- Thank Peter Dutton for No Blank Cheque on The Voice
- QLD: Do not attack parent rights and school choice
- Thank Senator Jacinta Price for opposing the divisive ‘Voice’
- Tell Mosman Council: Don't cancel Christmas!
- Thanks for Protecting Freedom of Speech
- Tell the SA Premier: Keep the Lord’s Prayer
- SA: Hands off the Lord’s Prayer
- NT: Stop attack on faith schools in the NT
- Keep using Mother and Father
- WA: Stop Zero Oversight To WA Emergency Powers
- Victoria – the Anti-Christian State
- WA: Defend Religious Freedom In WA
- Thank Anthony Albanese for keeping the Monarchy on our money
- Thank the Australian Catholic Bishops Conference for standing up to gender ideology
- QLD: Sophie's Law - Does the Queensland Government have a heart?
- Thank UAP Senator for standing up to radical identity ideology
- Stop abortion attack on religious hospitals
- Ask Albanese: When will you deliver $275 power bill cut?
- Stop the Killing in the Territories
- Keep opening the Senate with the Lord’s Prayer
- Coalition’s refreshing new voice of truth
- Tell the Manly Sea Eagles: Stick to footy - Ditch the LGBT propaganda
- Keep Christmas Day For Jesus
- Save Freo from “All Ages Drag Show”
- Tell MPs: We need a National Strategy to safeguard babies
- Say No to giving our Sovereignty away
- Say No to changing Birth Certificates in QLD
- Tell the woke NSW Premier: Keep the NSW flag – ditch the identity politics
- Introduce Miles Law to Protect Life in QLD
- QLD: Holding the QLD Premier to Account
- VIC: Andrews government divides children
- Adam Bandt disrespect for Australia, Australians and our Flag
- Keep Christian Chaplains in Schools
- Albanese to Ditch the Queen
- Keep Doors on School Toilets
- Tell the Breastfeeding Association: Do not cave to woke trans ideology
- Keep Blokes out of Women Sport
- Keep Australian Children Safe from Harms
- Mr Morrison - Can you help?
- Defund the UN over extreme abortion and gender ideology stance
- Tell Anthony Albanese: Protect Children from Trans Activists
- Protect Australians: Say no to hard drugs
- Stop Big Tech from Silencing Australians
- Tell MPs: Save Women’s Sport
- Time to Deliver on Religious Discrimination
- End Discrimination based on COVID19 Vaccination Status
- VIC: Act now to save Christian schools’ right to employ
- Tell MPs: Protect Free Speech
- Have your say in stopping kids’ access to online porn
- VIC: Act now to stop prostitution being decriminalised
- The ABC needs fixing
- WA: Free to Change: Stop McGowan’s therapy ban
- VIC: Act now to stop a second failed drug-injecting centre
- Act now to stop trans drugs for children
- Act now to stop Patten’s reckless changes to vilification laws
- Born Alive Bill
- Gambling Campaign
- Past Campaigns
- Events
- Contact
- 365Life
- Mother of the Year Awards
- Media Releases
- Little Music Church
- Australian Christian Man of the Year Awards
![]()
YOUR GUIDE TO CURRENT ISSUES ON FAMILY, LIFE AND SOCIETY
 Donate
Donate Subscribe to our weekly newsletter to be kept up to date with the work FamilyVoice Australia is doing in our nation ![]()
-
Home

- News
News

The Left has always been underhanded with its use of language.
For a long time, Left-wing social reconstructionists have understood the power of words in attractively packaging political ideologies detrimental to the wellbeing of society and the freedoms that we enjoy. One obvious example is the frequent use of the deceptive phrase “marriage equality” rather than “homosexual marriage.”
As the gender confusion movement is founded on the basis of the lie that there are more than two genders, it feels the need to police those who bring biological reality back into the public conversation.
This is where two trendy terms “misgendering” and “deadnaming” – which, of late, are being used as weapons in the cultural Marxists’ efforts to hijack language - come into the game.
Earlier this week, in an effort to further crackdown on free speech, Twitter banned “misgendering” and “deadnaming.”
“Misgendering” is when someone refers to another using a pronoun associated with that person’s real gender and not their fake gender.
According to GenderTerror.com:
Intentionally misgendering someone is an attack. Our genders and identities are constantly up for debate and misgendering a trans* person is a reminder of that. Misgendering us is a reminder that our identities are considered fragile, something to be bent and broken to the will of the cis people who wish to abuse us. When someone cannot get to us, they go in through our hearts and our minds. They dig deep. Sticks and stones may break our bones, but words can leave just as permanent scars. This includes something such as perpetual misgendering and denial of one’s self.
Not surprisingly, the gender confusion movement paints itself out to be the victim when, in reality, it is the perpetrator punishing dissenters who refuse to be coerced into using approved “transgender” speak.
How about “deadnaming”? That’s when a person who is confused about their gender is called by the name they were given at birth instead of the name that is associated with their new fake gender.
The Huffington Post, an unashamed gender-confusion-peddling tabloid, claims that “deadnaming a trans person is violence.”
Hearing or seeing one’s old name can induce a visceral sense of terror that no matter how much progress one makes in their transition, the person they used to be (or pretended to be) is still there.
If it were just cultural policing of these “offences” that would be bad enough. But more concerning is that the gender confusion movement is seeking to co-opt the state into policing truth and undermining our right to free speech through the invention and manipulation of language.
As George Orwell wrote in the classic manifesto 1984, “The further a society drifts from the truth, the more it will hate those that speak it.”
In the face of such a hostile and ruthless movement we must remain strong and continue to speak truth to power.

The voters of Victoria have a momentous opportunity this Saturday to rid the State (and the nation) of truly wretched euthanasia legislation. The current law is due to come into effect next year, but it will be repealed if enough pro-life candidates are elected.
Since the major parties tend to treat the life issues (such as abortion and euthanasia) as conscience votes, it is imperative that voters choose candidates, not major parties, when voting. The major parties have some candidates who are pro-euthanasia and others who are pro-life.
Your careful and considered vote on Saturday could make all the difference.
Candidates we understand to be pro-life include the following:
FOR THE LOWER HOUSE (THE HOUSE OF ASSEMBLY):
ALP: Anthony Carbines, John Eren, Marlene Kairouz, James Merlino, Tim Richardson, Natalie Suleyman.
Australian Liberty Alliance: Siobhann Brown.Democratic Labour Party: Arthur Bablis, Victor Bennett, Jennifer Bowden, Kathryn Breakwell, Stephen Campbell, Dermot Connors, Fi Fraser, Liz Freeman, Sami Greiss, Nathan Keen, Des Kelly, Leon Kofmansky, Helen Leach, Michael Long, Ross McPhee, Peter Mulcahy, Peter O’Brien, Tony O’Brien, Peter Phillips, Joseph Purtill, Edward Sok.
Liberals/Nationals: Neil Angus, Brad Battin, Gary Blackwood, Tim Bull, Neale Burgess, Robert Clark, Peter Crisp, Michael Gidley, David Hodgett, Andrew Katos, Tim McCurdy, Cindy McLeish, Danny O’Brien, Michael O’Brien, John Pessuto, Richard Riordan, Dee Ryall, Steph Ryan, Ryan Smith, Tim Smith, David Southwick, Bill Tilley, Heidi Victoria, Nick Wakeling, Peter Walsh, Graham Watt, Kym Wells.
Independent: Russell Northe.
FOR THE UPPER HOUSE (THE LEGISLATIVE COUNCIL):
ALP: Melina Bath, Nazih Elasmar, Adem Somyurek.
Australian Liberty Alliance: Indhira Bivieca Aquino, Mark Brown, Francine Cohen, Terri Franklin, Russell Gomez, Daniel Jones, Kaylah Jones, David Maddison, Daniel Macdonald, Ewan McDonald, Kenneth Nicholls, John Reisner, Ralf Schumann, Royston Wilding, James Wylie, Avi Yemini.
Democratic Labour Party: Benjamin Cronshaw, Jackie Gwynne, John McBride, Chris McCormack,
Larry Norman, Jeremy Orchard, Padraig O'Hea, Michael Palma, Mark Royal, Peter Stevens, Lucia De Summa, Joel van der Horst, Walter Villagonzalo, Jarred Vehlen.
Liberals/Nationals: Georgie Crozier, David Davis, Bernie Finn, Margaret Fitzherbert, Wendy Lovell, Josh Morris, Craig Ondarchie, Luke O’Sullivan, Inga Peulich, Gordon Rich-Phillips.
Shooters & Fishers: Jeff Bourman, Daniel Young.
Independent: Rachel Carling-Jenkins
Authorised by C. Newington, FamilyVoice Australia, 4th Fl, 68 Grenfell Street, Adelaide SA 5000

Bibi’s crime and subsequent acquittal
The coverage of Asia Bibi’s recent trial, acquittal and release has been fairly comprehensive - but since her release the trail has gone quiet. Where is she and in what circumstances?
Asia Bibi is a Christian mother of five children, from very poor circumstances. She was working in a field with other local women when a dispute arose because she was accused of drinking from the same vessel as the other (Muslim) women. This dispute led to an accusation that she had insulted Mohammed.
In Islam a non-believer is not permitted to touch or share a drinking vessel with Muslims as Islam teaches that they are unclean. This law led to the angry scene in the field which resulted in her arrest and imprisonment for over eight years.
Her imprisonment was in solitary confinement and she prepared her own food because of the constant threat of poisoning.
Recently the Pakistani Supreme Court acquitted Asia owing to a lack of substantial evidence to support the accusation of blasphemy against Mohammed. There was the expected outrage which led to the conditions that she is not allowed to leave the country and further legal action against her may yet occur. Because of the threats to her life, she was not released but moved to an undisclosed prison destination for her own protection.
Out of prison but not yet free
Then one night it is alleged that a vehicle came to the prison and whether it was connected to her release or not cannot be substantiated but when daylight came, Bibi was no longer in the prison. Her location now is unknown and remarkably she has remained undiscovered.
To Australians who enjoy the great freedoms of faith, association and expression, the case of Asia Bibi is almost beyond comprehension.
Western nations that enjoy Christian foundations are keen to uphold the rule of law and we take seriously such articles as the Universal Declaration of Human Rights.
That Declaration includes the right of freedom of religion: “Everyone has the right to freedom of thought, conscience and religion; this right includes freedom to change his religion or belief, and freedom, either alone or in community with others and in public or private, to manifest his religion or belief in teaching, practice, worship and observance” (Article 18).
While Pakistan was one of the first signatories to the Declaration, it is no simple matter to incorporate the values of the Declaration into the culture of Islamic nations. To conservative Muslims, Islamic Law (Shariah) is above all other jurisprudence. It is above the law of the land and the Universal Declaration of Human Rights.
Shariah is not just a religious or moral influence. It is a legislative reality that regulates daily life and practice well beyond rituals such praying and washing. It specifically regulates relationships between Muslims and non-believers with a very strong assumption about the supremacy of Islam.
When Muslims are in the social minority as they are in Australia, there is an acknowledgement of the laws of the land and general adherence. But for the traditionalists, the Islamic ideal is always in mind - that society will change when Islam gains the ascendancy.
As for the plight of Asia Bibi and her family, the fact that she has not been discovered and lynched is a very good sign. But Asia and her family need more. We might wish that the Pakistani government would securely deliver Asia Bibi and her family to safety in a Western nation but this story is not likely to follow the Western path.
Calls for Asylum
Several Western governments are under pressure to offer asylum to Asia Bibi and are weighing the political and social implications of intervening. What will be the reaction of local Muslims in such a host country? How will authorities keep the family safe? Can the Christian church be relied upon to provide social support without showcasing Asia Bibi? Will militant Islamists react with violence and murder? What would happen to relations with other Muslim majority nations who provide oil, buy technology and provide employment to the West?
Meanwhile, Asia Bibi and her family are from among the very poor. They are virtually illiterate and have no language apart from their mother tongue. If their freedom and safety is to be accomplished it would be better for it to happen in a way that causes as little disruption and loss of face as possible.
Call for prayer and discreet diplomacy
While there is a place for political pressure, let us not neglect the value of discreet approaches and above all Christian prayer. And as we pray, remember that the freedoms we enjoy are very fragile and require careful protection.
Although Australia endorses the Universal Declaration of Human Rights and we have pledged ourselves to defend freedom, we are seeing legislation emerge that will undermine our commitment to freedom of religion.
Christian prayer is an often misunderstood practice. The assumption of some is that it is like a spiritual generator that increases ‘spiritual mass’ in a given situation. So it follows that the more we pray the greater the mass, the greater the result. I suggest that prayer is the personal engagement of a Christian with God through Christ. In prayer, God is very much the Senior Partner. We do not come to demand or even persuade. We come to listen and learn his position on any given matter, and then to align ourselves with Him in faith.
The term ‘vigil’ reminds us that prayer is waiting and watching for God’s leading in a given situation such as Asia and her family. Some think prayer is like writing an email, pressing ‘send’ and assuming the matter is now resolved. It may be but prayer is about changing the one who prays as well as the pressing need. In this case, Bibi’s need is making us mindful that religious freedom is a great treasure and an inalienable human right for all, not just ‘for us’. Perhaps we have been too casual about it, too thankless and too irreverent.
It may not be your habit or tradition, but I’m suggesting you light a vigil candle (or set up a little tea candle) in the window of your home, your church, on your desk at work or in some place to remind you to pray and where others may see it. Place her name there and make space in your life to remember her and her family until we know that they are safe – whether in the arms of loving friends… or in the arms of Jesus which is far safer.
Here are some prayers to reflect upon in this vigil:
- Our Father, we ask you to intervene for Asia Bibi and her family. Grant them safety and security so they may live peaceful and productive lives.
- God of the Nations, we pray for influence to come upon the nation of Pakistan that they would take seriously their human rights obligations.
- Father, we acknowledge we have not always valued the freedom and equality of all citizens as we ought. As our own nation becomes increasingly complex socially we ask you to teach us all to manage our differences respectfully and successfully.
- We give thanks for our freedoms and recognise they come in large part from the Christian heritage of previous generations. Help us to serve you and our nation well so that those who succeed us will benefit from our faithfulness to Christ and from how we lived and communicated his good will for our society.

FamilyVoice Australia is deeply disappointed that WA Health Minister Roger Cook announced a euthansia bill and pro-euthanasia expert panel.
The panel's so-called “community consultation” will rely on incomplete and flawed research as the Sanderson End of Life Choices report which fails to mention data on overseas experiences such as in Oregon, USA.
"A government that sends an inherently conflicting message that doctors can both kill and care for vulnerable dying patients is fundamentally not to be trusted," said WA State Director Darryl Budge.
"Mr Cook fails to realise that doctors will not have a legal obligation to follow through with high quality palliative care.
"Furthermore, doctors themselves will most likely choose the path of least cost and encourage patients towards assisted killing.
"WA already has an above average suicide rate, recording 15.8 suicides per 100,000 people, compared with 12.6 nationally, in ABS figures released in September.
"Data from Oregon shows the suicide rate has climbed steadily since euthanasia was legalized in 1997 and in 2016 was 5% higher than the national average."
For all media enquiries, please contact Darryl Budge on 0468 454 507

By Darryl Budge
A new study on a 12,000-person dataset by the Institute for Family Studies has found that the happiest married people are faithful to one partner.
This is the first study to examine whether sexual history impacted the quality of marriages. Other studies have found that those who marry as virgins have the lowest divorce rates.
The study found that 71% of men and 64% of women with one lifetime sexual partner were “very happy” in their marriages. This slid below 65% of men and 60% of women who had 2 or more lifetime sexual partners.
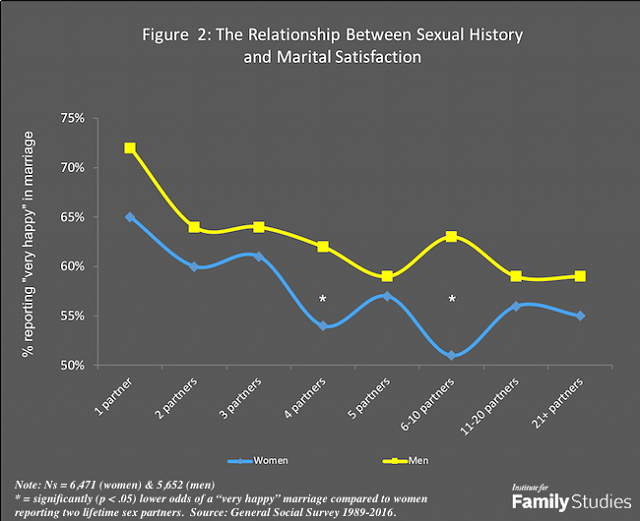
The results of the IFStudies.org study show a dramatic decline in marital happiness for those with two or more lifetime sexual partners.
Why should we be surprised by this? Detaching sex from marriage, and committed lifelong love from sex, has been hurting people for thousands of years. Eventually we must confront reality – something which no study or philosophy can reverse.
Moral psychologist Jonathan Haidt (who is not a Christian) has observed in his book The Happiness Hypothesis, “True love exists, I believe, but it is not—cannot be—passion that lasts forever. True love, the love that undergirds strong marriages, is simply strong companionate love, with some added passion, between two people who are firmly committed to each other.”
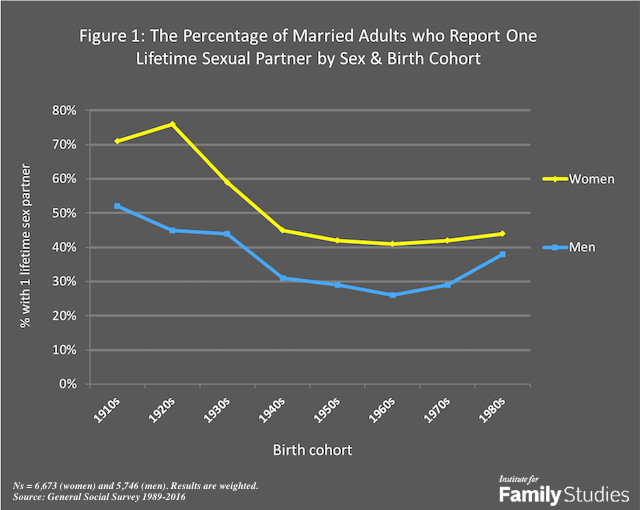
This graph of the U.S. General Social Study dataset shows the number of people with one sexual partner has declined dramatically over the last 100 years.
The Bible says in 1 Corinthians 13 that "love is not self-seeking... it always protects, always trusts, always hopes, always perseveres."
God's Word also warns in Proverbs 6:32 that immorality is self-destructive: "He who commits adultery lacks sense; he who does it destroys himself."
"Every other sin a person commits is outside the body, but the sexually immoral person sins against his own body," says 1 Corinthians 6:18.
There is no running from reality.
FamilyVoice Australia upholds Christian values and the family: permanence of marriage, sanctity of human life, primacy of parenthood and limited government.
Subscribe to our award-winning publications!
Don't miss out on quality research and news that will equip you to face the culture wars.
Society is suffering from ‘progressive’ ideas.
Join the growing movement of young people daring to be counter-cultural.